Perfect is the enemy of good.” This phrase is derived from a French proverb, yet it is most often attributed to the famous French writer Voltaire. It observes that those striving for perfection are their own worst enemies.1 Indeed, perfectionism is overly demanding of those who struggle with it. With its irrational and impossible demands, perfectionism can cause anxiety, create high levels of distress that inhibit learning and performance, damage relationships, and diminish the quality of life for otherwise highly competent and dedicated individuals. Perfectionism can be the main problem that leads someone to seek therapeutic services from a mental health professional. Perfectionism can also appear in conjunction with several mental health conditions such as depression, eating disorders, anxiety disorders, or obsessive-compulsive disorder (OCD). In someone with OCD, perfectionism around religious or moral content is called scrupulosity.
This article begins by briefly defining healthy (adaptive) and unhealthy (maladaptive or toxic) perfectionism (see also “Understanding Perfectionism” herein) and then illustrates the ways unhealthy perfectionism influences those who struggle with it. These discussions prepare the reader for deeper explorations of gospel and clinical perspectives on healing from unhealthy perfectionism. The gospel focus on healing will highlight three Christian doctrines: we don’t perfect ourselves, we become perfected in Christ, and perfection comes only after the Resurrection. The clinical focus on healing from perfectionism will highlight treatment from the cognitive perspective. The article will conclude with a brief discussion of the similarity between the two treatment approaches.
Please note that the personal stories or quotes from those struggling with perfectionism used throughout this article are shared with permission.
Healthy Perfectionism and Unhealthy Perfectionism2
Healthy Perfectionism
Perfectionism can be both adaptive and maladaptive.3 Elder Neal A. Maxwell of the Quorum of the Twelve Apostles taught, “There is a difference, therefore, between being ‘anxiously engaged’ and being over-anxious.”4
People who are “anxiously engaged” may be what social-science researchers call adaptive perfectionists or positive perfectionists. Those with adaptive perfectionism set high standards for themselves—not out of fear of negative evaluation or failure but because they are seeking to reap the positive consequences of success.5 As a result, they are not necessarily disturbed when they are unable to meet their standards. When a person with healthy perfectionism fails, they engage in positive, helpful behaviors such as tackling their problem directly, trying again, adjusting standards, working harder, or simply accepting the situation if there is no reasonable way to (or reason to) address the failure.6 If they do struggle when they fail,7 they are able to work through the situation by responding with flexibility and resiliently move forward to adapt to new circumstances. For example, a college student who did not get into their chosen major of study could reassess their interests and strengths and then select a new major. This new major may end up setting them on a more fulfilling path than the one they had originally selected for themselves. Indeed, researchers have found that working to meet high standards has been associated with higher self-esteem and life satisfaction.8
In religious worship, the anxiously engaged are conscientious about living their religion in its fullness in all areas of their lives.9 Researchers described this process: “Healthy religious observance . . . is generally typified by . . . moderate and flexible approaches to most areas of religious belief and practice, viewing perfect adherence as more of an ideal than as an imperative that is necessary to avoid subjective guilt or the threat of severe punishment.”10 You’ve likely had conversations with many such people and noticed their strong faith and ability to come to a healthy, balanced resolution about their difficulties, even in the face of disappointment in themselves or their own behavior.
Unhealthy Perfectionism
The “overanxious” may struggle with unhealthy perfectionism, a generalized anxiety disorder, or a more severe mental health concern, such as OCD. This unhealthy perfectionism is a frantic effort to live error-free: “the tendency to believe there is a perfect solution to every problem, that doing something perfectly (mistake free) is not only possible, but also necessary, and that even minor mistakes will have serious consequences.”11
Those with unhealthy perfectionism that are religious are generally very loyal to God, committed to keeping his commandments, and trying to perfectly follow him, but when they fail to meet their own unattainably high standards, they are overcome by anxiety, panic, and obsessive rumination about their perceived failures. For them, failure is not just about failing a task (for example, not getting a perfect score on an assignment); failure means they are a failure as a person—they feel unlovable and of no worth. For those struggling with unhealthy perfectionism, the consequences of failure are disastrous. Thus, instead of actively engaging in their problems, they tend to avoid them to protect themselves from their negative feelings.12
Negative perfectionism is associated with the “tendency to view the world in black-or-white terms” and with an intolerance and distrust of others—including God.13 A therapy client, a male in his late teens, expressed his fear this way: “If the worst happened it would mean I’m not a good person and that God doesn’t care about me. It means that God would send me to hell and that he hates me. At the judgment day he’d tell me: ‘you were a good person except that one thing you did.’ So, then I’m going to hell.”14 One researcher explained that those struggling with unhealthy perfectionism have “unrealistic expectations with an unhealthy preoccupation with faults, weaknesses, mistakes, and sins.”15 He summarized, “Thus the problem with perfectionism is not high expectations; it is neurotic expectations that are unrealistic and oppressive.”16
The overanxious person’s faith may be strong and equal to the faith of anxiously engaged people; they are typically wonderful, dedicated disciples! Yet their unhealthy perfectionism paralyzes them spiritually with a cloud of anxiety. Elder Boyd K. Packer taught that “our physical body is the instrument of our spirit,” and that it houses “delicate physical senses which have to do with spiritual communication.”17 Anxiety disrupts these “delicate physical senses” because it causes our brains to release chemicals that create physiological responses, which cloud our reception of the Spirit. It can even be difficult to tell the difference between what our body feels because of spiritual promptings and what it feels because it is releasing stress hormones.18
Unhealthy perfectionism does not enhance a person’s quality of life or motivate them to improve; instead, it decreases their quality of life and inhibits true personal growth and development. Elder Jeffrey R. Holland counseled, “I would hope we could pursue personal improvement in a way that doesn’t include getting ulcers or anorexia, feeling depressed or demolishing our self-esteem. That is not what the Lord wants. . . . My brothers and sisters, except for Jesus, there have been no flawless performances on this earthly journey we are pursuing, so while in mortality let’s strive for steady improvement without obsessing over what behavioral scientists call ‘toxic perfectionism.’”19 The process of breaking free from unhealthy perfectionism can include both gospel and clinical approaches.
Gospel Perspectives on Healing from Unhealthy Perfectionism
The gospel of Jesus Christ offers relief and freedom from the trap of unhealthy perfectionism. This freedom is rooted in doctrine. Fully understanding the doctrine—intellectually and emotionally—can be tremendously freeing. I wish to highlight three doctrinal principles that can promote healing from unhealthy perfectionism: (1) we don’t perfect ourselves, (2) we become perfected in Christ, and (3) perfection comes only in and through Jesus Christ after the Resurrection.
We Don’t Perfect Ourselves
Those with unhealthy perfectionism “cannot forgive [themselves] for not being perfect.”20 Yet as mortals, by definition, we are incomplete and imperfect. So demanding an error-free performance with no grace for mistakes is completely futile and absolutely maddening. The restored gospel of Jesus Christ teaches that we do not—we cannot—perfect ourselves. A survey of scriptural evidence illustrates this principle:21
Ephesians 2:8–9, “For by grace are ye saved through faith; and that not of yourselves: it is the gift of God: Not of works, lest any man should boast.”
2 Nephi 2:3, 6, “I know that thou are redeemed, because of the righteousness of thy Redeemer. . . . Redemption cometh in and through the Holy Messiah; for he is full of grace and truth.”
Alma 22:14, “And since man had fallen he could not merit anything of himself; but the sufferings and death of Christ atone for their sins, through faith and repentance.”
Alma 24:10, “And I also thank my God, yea, my great God, that he hath granted unto us that we might repent of these things, and also that he hath forgiven us of those our many sins and murders which we have committed, and taken away the guilt from our hearts, through the merits of his Son.”
Alma 33:11, 13, “For in thee is my joy; for thou hast turned thy judgments away from me, because of thy Son. . . . Thou hast turned away thy judgments because of thy Son.”
Helaman 14:13, “And if ye believe on his name ye will repent of all your sins, that thereby ye may have a remission of them through his merits.”
3 Nephi 26:5, “If they be good, to the resurrection of everlasting life . . . according to the mercy, and the justice, and the holiness which is in Christ.”
Doctrine and Covenants 76:69, “These are they who are just men made perfect through Jesus the mediator of the new covenant, who wrought out this perfect atonement through the shedding of his own blood.”
Doctrine and Covenants 109:53, “Inasmuch as they will repent, thou art gracious and merciful, and wilt turn away thy wrath when thou lookest upon the face of thine Anointed.”
Psychiatrist Ian Osborn has developed what he calls a Therapy of Trust.22 In the Therapy of Trust, a person transfers responsibility for their fears onto God, recognizing that believers are not responsible for perfecting themselves. As Christians, we are familiar with the image of Jesus knocking on a door, as offered in the book of Revelation: “Behold, I stand at the door, and knock” (Rev. 3:20). In the Therapy of Trust, we open the metaphorical door and invite Jesus into our lives. We share our perfectionistic fears with him and give him responsibility for them. In essence, we are saying, “Here, Jesus, you look after this.”23
We Become Perfected “in Christ”
As the above scriptures and Therapy of Trust illustrate, it is not by our merit that we become perfect; it is through Jesus Christ.24 This doctrine is core to the belief of Christians. The Atonement works as we, imperfect mortals, join with a perfect Christ in a covenant relationship. It is then through his perfection and power (his merits) that we become perfected in him. The scriptures illustrate this companionship beautifully:25
Psalm 37:17, 24, 39–40, “The Lord upholdeth the righteous. . . . Though he fall, he shall not be utterly cast down: for the Lord upholdeth him with his hand. . . . But the salvation of the righteous is of the Lord: he is their strength in the time of trouble. And the Lord shall help them, and deliver them: he shall deliver them from the wicked, and save them, because they trust in him.”
Hebrews 9:14–15, “The blood of Christ . . . purge your conscience from dead works. . . . And for this cause he is the mediator of the new testament, that by means of death, for the redemption of the transgressions that were under the first testament, they which are called might receive the promise of eternal inheritance.”
1 John 1:7–9, “But if we walk in the light, as he is in the light, we have fellowship one with another, and the blood of Jesus Christ his Son cleanseth us from all sin. If we say that we have no sin, we deceive ourselves, and the truth is not in us. If we confess our sins, he is faithful and just to forgive us our sins, and to cleanse us from all unrighteousness.” (Obsessively trying to perfect oneself denies Christ’s refining role.)
Revelation 1:5, “Jesus Christ . . . washed us from our sins in his own blood.”
2 Nephi 2:3, 9–10, “Wherefore, I know that thou art redeemed, because of the righteousness of thy Redeemer. . . . Wherefore, he is the firstfruits unto God, inasmuch as he shall make intercession for all the children of men; and they that believe in him shall be saved. And because of the intercession for all, all men come unto God; wherefore, they stand in the presence of him, to be judged of him according to the truth and holiness which is in him.”
Moroni 10:32–33, “Yea, come unto Christ, and be perfected in him[;] . . . then is his grace sufficient for you, that by his grace ye may be perfect in Christ. . . . If ye by the grace of God are perfect in Christ, and deny not his power, then are ye sanctified in Christ by the grace of God, through the shedding of the blood of Christ, which is in the covenant of the Father unto the remission of your sins, that ye become holy, without spot.”
Perfection Comes Only In and Through Jesus Christ After the Resurrection
As mortals, we all sin, and we all make mistakes. Bradley R. Wilcox, second counselor in the Young Men General Presidency, taught, “Some mistakenly receive the message that they are not worthy to participate fully in the gospel because they are not completely free of bad habits. God’s message is that worthiness is not flawlessness. Worthiness is being honest and trying. We must be honest with God, priesthood leaders, and others who love us, and we must strive to keep God’s commandments and never give up just because we slip up.”26
Simply stated, we will not achieve perfection, in its most complete sense, until after the Resurrection. Becoming perfected in Christ is a journey of maturing, growing, and becoming like our Savior—a process only possible through his grace. This process extends well beyond this mortal probationary time into the eternities.
As a member of the Quorum of the Twelve Apostles, Elder Russell M. Nelson clarified the doctrine of perfection as it was taught in the New Testament and then explained its relationship to Jesus Christ.27 He first quoted Matthew 5:48, wherein the Savior implored: “Be ye therefore perfect, even as your Father which is in heaven is perfect.” Then Elder Nelson taught that the term perfect was translated from the Greek teleios, which means “complete,” and that it was an adjective derived from the noun telos, which means “end.” The infinitive form of the verb is teleiono, which means “to reach a distant end, to be fully developed, to consummate, or to finish.” Then Elder Nelson explicitly noted that “the word does not imply ‘freedom from error’; it implies ‘achieving a distant objective.’”28
After explaining the meaning of the word perfect, Elder Nelson taught: “Just prior to his crucifixion, [Jesus] said that on ‘the third day I shall be perfected.’ Think of that! The sinless, errorless Lord—already perfect by our mortal standards—proclaimed his own state of perfection yet to be in the future. His eternal perfection would follow his resurrection and receipt of ‘all power’ . . . in heaven and in earth.”29
In concert with this teaching, when the resurrected Savior ministered to the Nephites, he repeated the teachings he had given to those in his mortal ministry as recorded in the New Testament. However, he altered the wording of Matthew 5:48: “Be ye therefore perfect, even as your Father which is in heaven is perfect.” In 3 Nephi 12:48, Jesus Christ now included himself along with the Father, as one who was perfect: “Therefore I would that ye should be perfect even as I, or your Father who is in heaven is perfect.”
Then Elder Nelson summarized:
Brothers and sisters, let us do the best we can and try to improve each day. When our imperfections appear, we can keep trying to correct them. We can be more forgiving of flaws in ourselves and among those we love. We can be comforted and forbearing. The Lord taught, “Ye are not able to abide the presence of God now. . . ; wherefore, continue in patience until ye are perfected.”
We need not be dismayed if our earnest efforts toward perfection now seem so arduous and endless. Perfection is pending. It can come in full only after the Resurrection and only through the Lord.30
In a later message, Elder Nelson counseled: “Be patient with yourself. Perfection comes not in this life but in the next life. Don’t demand things that are unreasonable but demand of yourself improvement. As you let the Lord help you through that, He will make the difference.”31 This process occurs through the grace of our Savior Jesus Christ. It is by his power, his merits, and his perfection that we are ultimately saved.
Facing doctrine as it is taught, rather than as it is influenced by negatively biased unhealthy perfectionism, is freeing! Christ is the answer! A person does not need to try harder, work harder, avoid mistakes, or control everything or everyone else in their lives. It is faith in Christ and a willingness to come unto him in humility that enables his power. His power, not ours, will save: “And he said to me, My grace is sufficient for thee: for my strength is made perfect in weakness” (2 Cor. 12:9).
Clinical Perspectives on Healing from Unhealthy Perfectionism
Examining the doctrines as they are taught will help change one’s negative focus, perspective, and view. Strategies that encourage flexibility in this way are part of a clinical treatment process that providers call cognitive restructuring.
Cognitive restructuring is a preeminent strategy in the treatment of unhealthy perfectionism. Through cognitive restructuring, a person learns to identify and dispute errors in their thinking. These errors lead to irrational thoughts and beliefs known as cognitive distortions.32 While studying relevant gospel doctrines in an emotionally open manner can shift and restructure distorted thoughts to some degree, research-based therapeutic treatments for perfectionism should also be implemented.
Cognitive Theory of Perfectionism
Before exploring treatment strategies, it is helpful to understand the premises of the cognitive theory of perfectionism. According to the cognitive theory, perfectionism stems from biased beliefs, assumptions, and predictions.33 These biases stem from distortions or inaccuracies in a person’s beliefs.
Those with unhealthy perfectionism hold a variety of self-defeating beliefs. These beliefs are “self-esteem equations that tell you what you need to be or do in order to be a worthwhile human being.”34 This performance perfectionism includes a belief that if someone fails to reach a goal or make a mistake, they will be worthless. Additionally, they can involve three processes. (1) Perceived perfectionism is a belief that others won’t respect you if they see that you are flawed. This is referred to as socially prescribed perfectionism (see pp. 15–16). (2) Achievement addiction means a person’s self-esteem is based on their intelligence, skill, talent, successes, and productivity. (3) Approval addiction is a belief that everyone needs to approve of who one is or what one is doing to be worthwhile.35
The cognitive theory for perfectionism also examines a person’s core beliefs—what therapists and researchers call schemas. These core beliefs are a person’s deepest ideas about themselves. These ideas are central to who they perceive themselves to be and are strongly held, tending to be rigid and inflexible.36 The most common core beliefs seen in people with unhealthy perfectionism are beliefs about their own worthlessness and incompetence as a human being.37 These types of distorted core beliefs were illustrated in the client illustration in “Understanding Perfectionism” (see pp. 17–18) describing unhealthy perfectionism touching every aspect of their life.
Those struggling with unhealthy perfectionism also exhibit a host of distortions in their thinking process. These distortions naturally follow self-defeating core beliefs. While self-defeating beliefs are always present, these distorted thoughts tend to come up only when someone is upset.38 Distortion causes rigidity of thought, so the thoughts get more entrenched as time goes on.
Of all the thought distortions, one of the most relevant for perfectionism is dichotomous (black-and-white or all-or-nothing) thinking.39 Dichotomous thinking leads a person to view the world in extremes—the pendulum always swinging from one end to the other. When thinking is black and white, there is no room for gray area. Although black-and-white thinking has its place (certainly some things are morally and absolutely wrong), those struggling with unhealthy perfectionism are tormented by feeling they are a total failure with anything less than a perfect performance.
Other common thinking styles in unhealthy perfectionism include the following:
Selective attention in perfectionism means a person’s thoughts gravitate toward the negative, and the person generally ignores anything positive. A person will habitually focus on negative aspects of themselves or their performance.40
Double standards is a thinking style in which a person holds “one set of unrelenting and difficult-to-achieve standards that they apply to themselves, and a more lenient set of standards for others.”41
Overgeneralizing means taking one mistake or flaw and extending it to other areas “as a never-ending pattern of defeat.”42 The overgeneralizing person concludes that if they are not perfect in one area, they are a failure in all areas.43
Should language, like “should,” “must,” and “ought,” is a form of self-criticism and judgment that those struggling with perfectionism use “like a whip as a way to motivate themselves and guard against poor performance.”44
The following distortions are seen in more general perfectionistic thinking styles: catastrophizing, emotional reasoning, labeling, personalization, mind reading, and predictive thinking. In catastrophizing, people frequently entertain the worst-case scenario with the ever-problematic question “What if?” Catastrophizing never fails to create significant anxiety. Furthermore, in OCD, this type of thinking is a significant contributor to the compulsion of rumination—replaying and analyzing thoughts over and over and over again. Catastrophizing is not concerned with what is likely or probable in a scenario, only what may be possible—even if it is a remote, almost-impossible possibility statistically equal to 0.00000001. Thus, someone who catastrophizes may avoid doing things because they imagine the worst possible scenario is bound to happen, even if it is highly unlikely.45
Emotional reasoning involves judging the truth of a scenario based on how the person feels about it—feelings override facts.46 An example of emotional reasoning may be “I feel like a failure, so I am a failure,” or “I feel unworthy, so I must be unworthy.”
Labeling involves generalizing “from a single flaw or shortcoming to your entire identity.”47 It doesn’t allow a person to be anything other than the label they have assigned. When not meeting some expected standard, they will assign negative self-labels such as dumb, loser, failure, useless, or unworthy.48
Personalization is related to self-blame. This is an overinflated sense of responsibility for every circumstance, even—and perhaps especially—when the responsibility is shared. The person does not consider all relevant factors contributing to a given outcome. “I have to fix this” or “It’s all my fault” are common indicators of personalization.49
Mind reading is an assumption that a person can tell what others are thinking, with a heavy bias assuming others are thinking negatively about them, even with no evidence.50
Predictive thinking, or fortune-telling, is a person making negatively biased predictions about how they will perform or how a scenario will unfold.51
In addition to thought distortions, those with unhealthy perfectionism hold a variety of self-defeating beliefs. These beliefs are “self-esteem equations that tell you what you need to be or do in order to be a worthwhile human being.”52 This performance perfectionism includes a belief that if someone fails to reach a goal or make a mistake, they will be worthless. Additionally, this belief involves three processes: (1) Perceived perfectionism is a belief that others won’t respect you if they see that you are flawed. This was referred to earlier as socially prescribed perfectionism. (2) Achievement addiction means a person’s self-esteem is based on their intelligence, skill, talent, successes, and productivity. (3) Approval addiction is a belief that everyone needs to approve of who one is or what one is doing to be worthwhile.53
Treatment Strategies for Toxic Perfectionism
As shown, self-defeating beliefs and distorted thought patterns of unhealthy perfectionism are focused on the negative. With this strong negative bias, the person engages in emotional and logical fallacies that cause their mental health to deteriorate. Treatment strategies aim to break rigid thinking patterns and create flexibility in a person’s thinking. More flexibility allows the person to modify self-defeating beliefs, creating healthier, reality-based beliefs that will help them grow and thrive. This is often done through cognitive restructuring and behavioral experiments, as described below. These interventions can be used across age groups, with slight modifications made for children and younger adolescents to simplify concepts and exercises. Some cognitive restructuring treatment strategies include challenging distortions, examining definitions, creating responsibility pie charts, and completing thought charts.
Challenging distortions. One cognitive method is to challenge perfectionistic distortions through Socratic questioning—a disciplined dialogue between individuals using a series of guided, open-ended questions to explore values and beliefs, some of which may be out of a person’s conscious awareness. In the psychotherapeutic process, therapists ask the client a series of ordered questions to guide the client to thought processes and behaviors that will help achieve therapeutic goals.54
To challenge the distortion of double standards, questions that could be asked include the following:
“Is it fair to have harsher rules for yourself that are different from your rules for everyone else?”
“What would you say to a friend who had a harder set of rules for herself than for other people?”
“What does holding double standards do to your self-esteem and mood?”55
Socratic questioning for overgeneralizing can include the following:
“How does it follow that someone’s worth as a person can be judged on one instance of not meeting a goal or making a mistake?”
“How is it that making a small mistake or error . . . can reflect on a person’s worth overall?”
“What do most people judge as important in making up a person’s worth?”56
To challenge the “should” mentality, questions may include the following:
“How does saying ‘should’ to yourself constantly make you feel? In what way does it impact on your sense of self?”
“What impact do you think it might have if you apply the sort of pressure you apply on yourself to a close friend?”57
This exercise is modifiable for a child or adolescent by asking questions more simply, using words the child uses and understands. For example: “Would you say that to your best friend?” or “Would you be mad at your best friend if they made that mistake?”
Examining definitions. In addition to challenging the distortions through Socratic questioning, you can examine the definitions of the words you are using to think about or describe yourself. Does the word you are using really mean what you perceive it to mean? What does it mean to be “a failure,” a “loser,” “useless,” or such? One researcher counseled:
Ask yourself what those labels mean. If you try to define what you mean . . . you’ll usually discover that one of four things is true:
This exercise is modifiable for a child or adolescent like the Socratic questioning above by asking questions more simply, using words and concepts the child uses and understands. This exercise can help children understand that pejorative terms like “loser” could never accurately or appropriately describe who they are.
Responsibility pie chart. A responsibility pie chart can help examine a perfectionistic, overinflated sense of responsibility. While in unhealthy perfectionism a person generally feels everything is their fault, a responsibility pie chart can clarify that there are typically many factors contributing to any outcome. This exercise helps to challenge faulty assumptions and shame while promoting cognitive flexibility. Those struggling with unhealthy perfectionism learn the important message that one person just doesn’t have that much power!
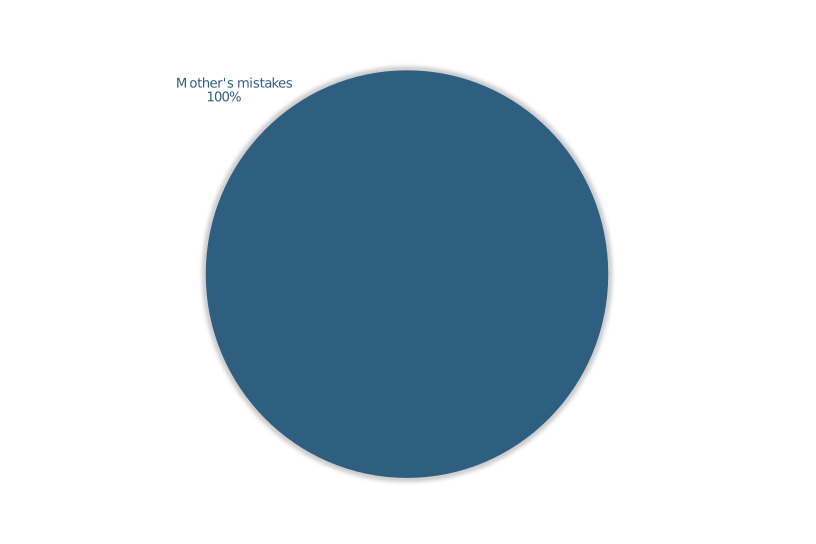
For example, one client, a married woman in her sixties, struggled with unhealthy perfectionism around a daughter’s estrangement from the family. Although this daughter cut off relationships with other family members prior to severing her relationship with her mother, this mother could not get over the unhealthy perfectionistic belief that it was all her fault because she had made mistakes as a mother. In her view, responsibility for the estrangement was one hundred percent on her shoulders—and thus, she was responsible for fixing it (getting the daughter to reconcile), or else she would be accountable to God for failing in her role as a mother. When it became clear over many years that she could not fix it, she tormented herself by continuing to analyze and ruminate about what she could or should or ought to do to reconcile with her daughter.
If we were to complete a responsibility pie chart for this client on how her unhealthy perfectionism viewed the situation, it would look like the one in figure 1. In this figure, there is one, and only one, factor to account for the daughter’s estrangement—the mother’s mistakes. This view does not consider the good the mother did for her daughter throughout her life or the fact that she had other children who continued to maintain vibrant parent-child relationships with her. It also does not consider the daughter’s role in the situation. Her unhealthy perfectionism convinced her that she was simply a failure as a mother because she hadn’t always done everything perfectly.
Figure 1. Responsibility pie chart: Client example (a) from perfectionistic viewpoint.
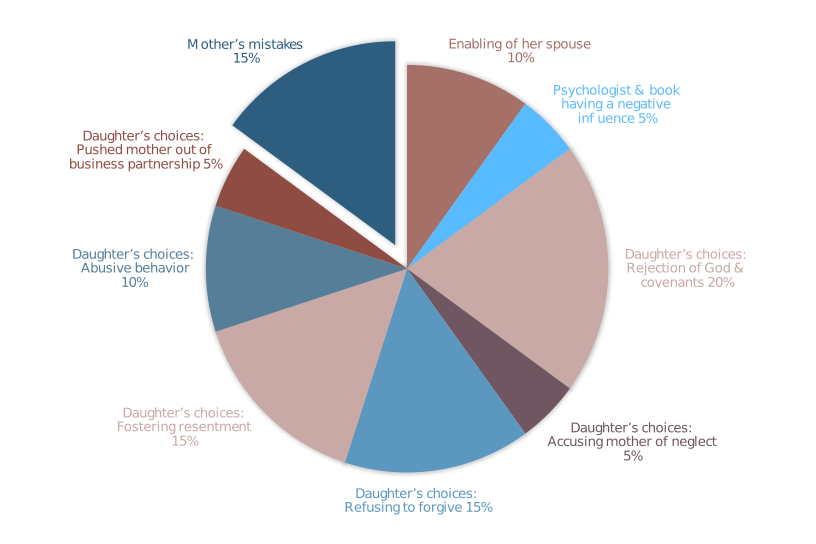
In a responsibility pie chart, a person works to combat an unhealthy perfectionistic view by listing all the potential contributing factors to a situation and guesstimating the probability that each factor contributed to the outcome. The point of this is not to know with perfect accuracy the factors and percentages, rather, the exercise is about learning to think more broadly and realistically about the issue. Many factors can contribute to family dynamics and specific family relationships. Figure 2 shows the work this client did to get a more realistic picture of the situation with her daughter.
Figure 2. Responsibility pie chart: Client example (b) from a realistic perspective.
Working to identify these dynamics, this client identified two outside influences on the daughter’s choice to leave the family and abandon her as a mother: (1) the enabling by the daughter’s spouse and (2) a psychologist who recommended a book that advised cutting people out of her life if they caused angst. The mother estimated that these two factors together equaled about 15% of the contribution to the estrangement outcome. She then identified a variety of choices this daughter made that contributed to the estrangement. If the daughter had made different choices in any of these areas, she recognized that the outcome could have been different. These additional choices, she surmised, added up to a huge 70% of the contribution! These choices included a rejection of her religious beliefs, accusing the mother of neglect, refusing to forgive, fostering resentment, acting abusively toward the mother, and pushing the mother out of their business partnership. Once this mother identified these factors (both the outside influences and her daughter’s choices) and estimated the contribution of each factor, 85% of the estrangement-outcome pie was already accounted for, leaving only about a 15% possible contribution to the outcome left for the mother’s mistakes.
Oh, how self-defeating beliefs begin to vanish when a person goes from believing one hundred percent of everything is their fault to believing they are responsible for only a portion of it! Responsibility pie charts can help a person shed an excessive sense of responsibility and accompanying shame and facilitate recognition of any cognitive distortions at play. With this more reality-based perspective, the person is more likely to be able to move forward in a healthy and productive way. After completing this exercise, upon reflection, this client commented: “What did I learn from that pie chart? I learned that it wasn’t all me.” This was a powerful commentary for someone who had suffered with unhealthy perfectionism for so many years. It opened her up to be able to explore the role of agency and face the hard truth that her daughter will always retain it—she cannot force her daughter to reconcile.
This exercise is also modifiable for a child or adolescent. When they are upset, feeling that everything is their fault, you can challenge them to think of two to four other things that may be involved in creating the situation or outcome. Drawing these factors out can be helpful and fun.
Thought charts. Distortion can also be challenged through the use of a thought chart, commonly called a thought record. An online search can provide many different examples of thought charts. A thought chart is a common psychotherapeutic tool that provides a person with a structured, organized approach to identify the presence of any distortion in their thinking and then encourage them to dispute the distortion with contrary evidence. This process leads the person to more reality-based thoughts and feelings that can be acted on more appropriately. For example, in unhealthy perfectionism, you can tease out the distorted belief that an error-free performance is necessary to be successful in life.
Working through an example with a thought chart will illustrate how this process can be helpful to perfectionistic individuals. Figure 3 shows how a client who struggled with academic perfectionism (see “Understanding Perfectionism” in this issue) completed one of his thought charts.
A
Activating Event
I got a 17/20 on a technical accounting memo.
B
Belief
“I’m going to fail the class.”
“I’m never going to succeed in law school.”
“I’m a fraud.”
“I’m dumb.”
C
Consequences
Sadness
Shame
Embarrassment
Feeling worthless
Rumination
D
Dispute
17/20 = 85%. That’s a B on one assignment.
This technical accounting research class is substantially different from law school.
My identity is not solely defined by academic performance in a single class.
Missing 3 points does not constitute a failing grade.
I have a 4.0. I’m not dumb.
Even if I didn’t get an A in this class or keep my 4.0, I can still reach my goal of going to law school.
E
Eliminate
I’m performing well in the class even if I’m not performing perfectly.
This experience will help me perform better in law school.
I have so much to offer beyond just academics.
I’m human and I will make mistakes. That’s okay.
F
New Feeling
Flexible
Grounded
Honest
Authentic
Confident
G
Go and Do!
I’ll keep trying my best without obsessing over my shortcomings.
I will invest in all areas of my life.
I will view imperfections as a gift.
Figure 3. Client thought chart, shared with permission.
Row A is the activating event. This is simply a place for the person to objectively record the event that triggered feelings of unhealthy perfectionism (shame, self-hatred, and so forth). For this client, the perfectionistic trigger was losing three points on an accounting assignment.
Row B is the personal belief that popped up about that event, or a person can identify automatic thoughts about the event. This client had four different automatic thoughts or beliefs about this activating event: “I’m going to fail the class; I’m never going to succeed in law school; I’m a fraud; I’m dumb.” These thoughts suggest that he is overgeneralizing, mentally filtering, fortune telling, and magnifying the problem. This client reported believing these thoughts about 90% at the height of this emotional trigger.
Row C represents the consequences caused by those beliefs or automatic thoughts. The consequences can be both emotional consequences (for example, I cried; I felt guilty; I was angry), or they can be behavioral consequences (for example, I left the room; I hit the wall; I cried; I isolated myself). This client listed the emotional consequences of sadness, shame, embarrassment, and feeling worthless. He listed one behavioral consequence of rumination. These three rows (A, B, and C) are simply a description of the person’s lived experience: (A) Something happened, (B) they had thoughts and beliefs about that something, and (C) consequences unfolded from their reaction to that something.
Row D is where the therapeutic exercise in flexibility begins. The person struggling with unhealthy perfectionism has spent much of their life looking for evidence to support the assumption(s) stated in row B (confirmation bias). Here they will learn to do the opposite and find evidence to disprove their beliefs and automatic thoughts. They will dispute the assumption in row B and give evidence for why the thought(s) is not one hundred percent true. Although this goes contrary to their regular thought patterns and may feel difficult, cognitive flexibility improves with practice, and the process becomes easier. Looking back to row D, we can see that he worked through evidence from a variety of angles to begin unseating the distorted thoughts in row B. His disputes were as follows: “17/20 = 85%. That’s a B on one assignment.” “This technical accounting research class is substantially different from law school.” “My identity is not solely defined by academic performance in a single class.” “Missing 3 points does not constitute a failing grade.” “I have a 4.0. I’m not dumb.” “Even if I didn’t get an A in this class or keep my 4.0, I can still reach my goal of going to law school.”
In row E, the client works to eliminate the distortion present in their previous row B thoughts by creating new, more reality-based thoughts. These summarize the essence of what they learned from their disputing beliefs in row D. As seen in this client’s example in row E, he created several summary statements about what he learned from the disputes he had written in row D: “I’m performing well in the class even If I’m not performing perfectly.” “This experience will help me perform better in law school.” “I have so much to offer beyond just academics.” “I’m human and will make mistakes. That’s okay.”
After processing through rows D and E, this client reported believing the thoughts in row B now only 10%, in contrast to believing them 90% when he was first triggered. As things shifted, the client recorded any new feelings he was having in row F, in contrast to the emotional and behavioral consequences he previously listed in row C. In row F, he recorded his improved mental state: “flexible, grounded, honest, authentic, and confident.” These are striking improvements over his earlier feelings of sadness, shame, embarrassment, and feeling worthless.
Once the therapeutic work in rows D, E, and F has been done, row G asks the person to consider what they will do going forward on this issue. It invites them to consider the question “What is my responsibility to honor the new feelings I created in row F?” This is a way to say, “Okay, now that I’m looking at it in a healthier way, and I feel differently, what am I going to do about it?” The person can put anything in this row that they feel is appropriate for their situation. You can see that in our example, the client decided, “I’ll keep trying my best without obsessing over my shortcomings,” “I will invest in all areas of my life,” and “I will view imperfection as a gift.” Deciding on new actions to take is a way of honoring the reality-based thoughts and feelings that the client just created. When behaviors align with these new feelings and values, the client experiences reduced stress and feelings of confidence and competence. At another time in his treatment journey, this client commented about the thought chart process: “I love [the] thought charts. These charts help ingrain healthy cognitive processes that breathe flexibility and contentment into my life.”59
This exercise is easily modifiable for a child or adolescent—help them identify their automatic thought (B), and then help them to think of evidence or disputes about why that thought is not one hundred percent accurate (D). You can make this a discussion, or they can write down the automatic thought (B) at the top of a paper, underline it, and then put all the disputes underneath it, making a bulleted list.
Behavioral Experiments
Behavioral experiments test core beliefs and help shift faulty cognitions as the person brings new information. Researchers explain, “Beliefs rarely change as a result of intellectual challenging, but only through engaging emotions and behaving in new ways that produce evidence that confirms new beliefs.”60 One treatment manual for mood disorders suggests, “The best way to increase the believability of your alternative or balanced thoughts is to try them out in your day-to-day life.”61
Contrast Experiments
For the treatment of unhealthy perfectionism, contrast experiments are recommended.62 In contrast experiments, clients can compare (or, really, contrast) how they already behave with a new way of behaving. For example, in academic perfectionism, the client may be exhibiting extreme and unhealthy study habits. Perhaps they procrastinate studying out of fear of not doing well, and then, in a frenzy, they stay up very late, studying into the early morning hours for a week prior to an exam. In a contrast experiment for their next exam, they can plan out their study time, study for a specified amount of time during each day, and then stop studying when they have completed their scheduled study time. They can evaluate how these two approaches to studying for exams affected their subjective quality of life (stress levels, sleep quality and fatigue, overall sense of enjoyment or misery), as well as the objective outcome of the exam (points or grade earned). They can then review this data and decide which way of studying for tests works best for them.
Shame-Attacking Exercises
My favorite behavioral experiments are shame-attacking exercises. In shame-attacking exercises, a person chooses to publicly and purposefully behave in a manner that triggers anxiety, shame, and embarrassment. Generally, they act in a manner that is not culturally expected (as long as it is not illegal, doesn’t hurt anyone, and doesn’t violate their values or long-term goals). The choice of shame-attacking exercises should line up to counter the person’s self-defeating beliefs or cognitive distortions.
One author explained the goals of shame-attacking exercises as follows: “The exercise has three goals. First and most important, is to provide experiences that prove you can act against your emotions, survive the discomfort, and behave as you planned despite unhealthy negative emotions. Second, it convinces you that even if people dislike or disapprove of you for your behavior, it is not awful, and you can stand their disapproval. Third and least important, it teaches us that most people do not even notice what we do, and we exaggerate the disapproval and reject we expect.”63
Three categories of shame-attacking exercises include (1) targeting specific perfectionistic issues, (2) publicly violating cultural expectations, and (3) boundary setting and assertiveness training.
First, some shame-attacking exercises can target the person’s specific perfectionistic tendencies. They can send texts with multiple purposely misspelled words. They can show up late for an appointment. They can attend a class, a therapy session, or another appointment without preparing or doing their assignments. They can tell a personal story to someone and leave out important details. They can fill out a questionnaire quickly rather than agonizing over every answer. They can admit to not knowing something. They can apologize when they make a mistake. And so on and so forth.
Second, some shame-attacking exercises involve violating some cultural expectations, which also trigger a host of emotions for someone struggling with unhealthy perfectionism. For example, a person can get in a crowded elevator and stay facing the back of the elevator instead of turning around to face the doors, as is generally expected. They can similarly ride an escalator facing backward toward the people behind them. They can turn up the music in their car when they stop at a red light next to another car, dance in their seat, and sing at the top of their lungs. They can approach people in a crowded store to survey them on a topic. They can button their shirt or blouse with the buttons mismatched so it hangs crooked. They can wear mismatched earrings. They can go to an important meeting with a big stain on the front of their shirt.
Last, shame-attacking exercises can also be serious practice with boundary setting or assertiveness training. The person can politely offer a differing opinion with a person of authority. They can politely ask for something they need without apologizing, being honest with people about what they need. They can bargain for a better price on a product they are purchasing. They can say “no” to a request from someone if they don’t want to do it. They can ask someone for help, even though they don’t know them well.
For children or adolescents, any behavioral experiments, such as the shame-attacking exercises just described, can be easily adapted by designing exercises that are interesting, creative, and even fun or silly. This approach motivates the child to remember to do them and be more willing to try them out. For example, most would find it risky but also a bit exciting to be challenged to talk to strangers at a store. The tension between the risk and excitement of doing something new and unexpected would be enticing to them. Curiosity would make them feel like they just have to do it so they can see what happens!
A Client’s Cognitive Treatment for Religious Perfectionism
A married man in his mid-forties with a large family struggled with extreme religious perfectionism and anxiety. His distress paralyzed him. He would stay in bed, hiding under his covers, unable to function. Although he was temple worthy, he avoided the temple for years because of plaguing thoughts about his imperfections. In treatment, he completed many thought charts and also did behavioral experiments. His thinking grew more flexible over time, and in that healthier state, his distress lessened, and he found more joy in life.
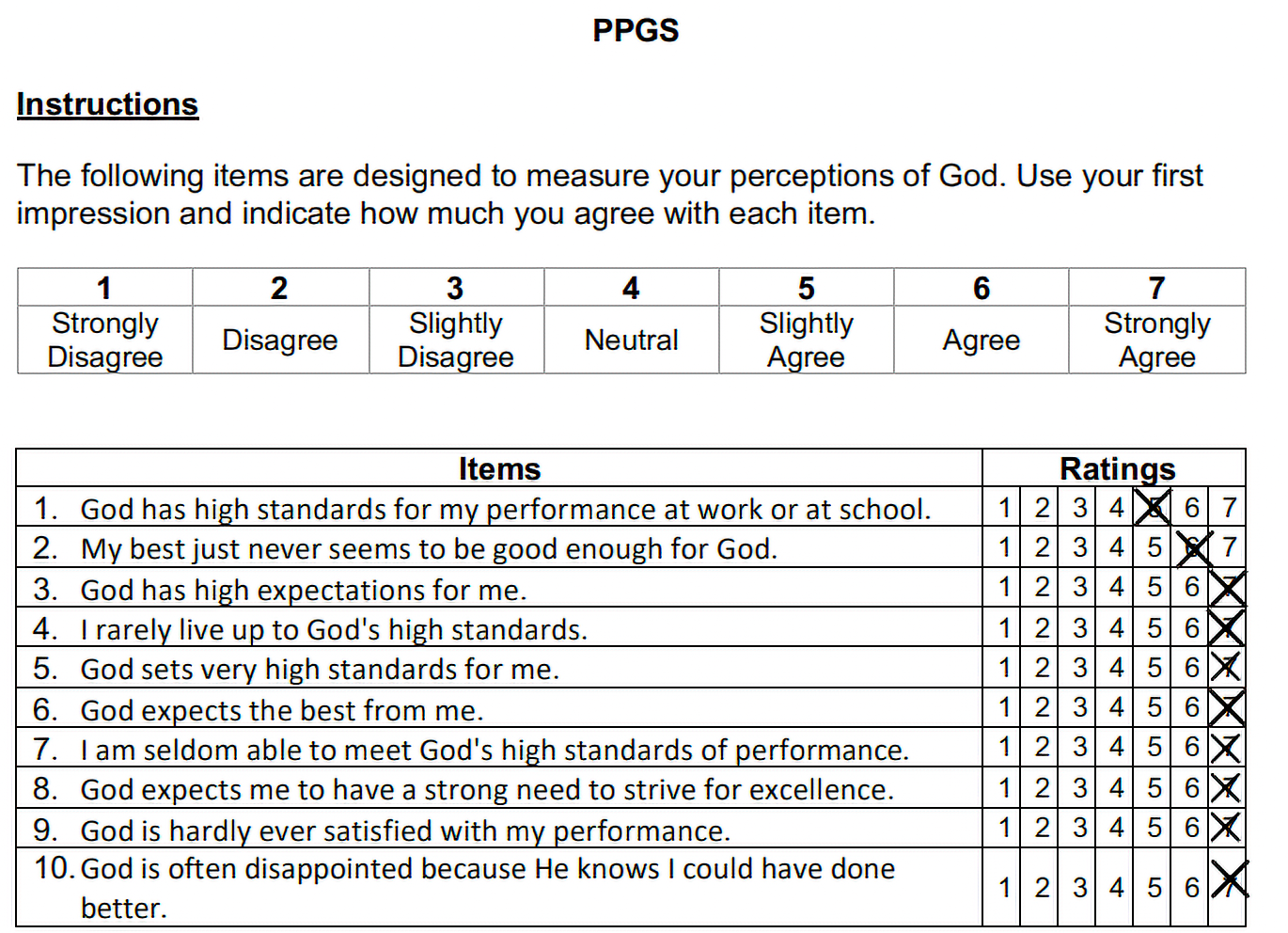
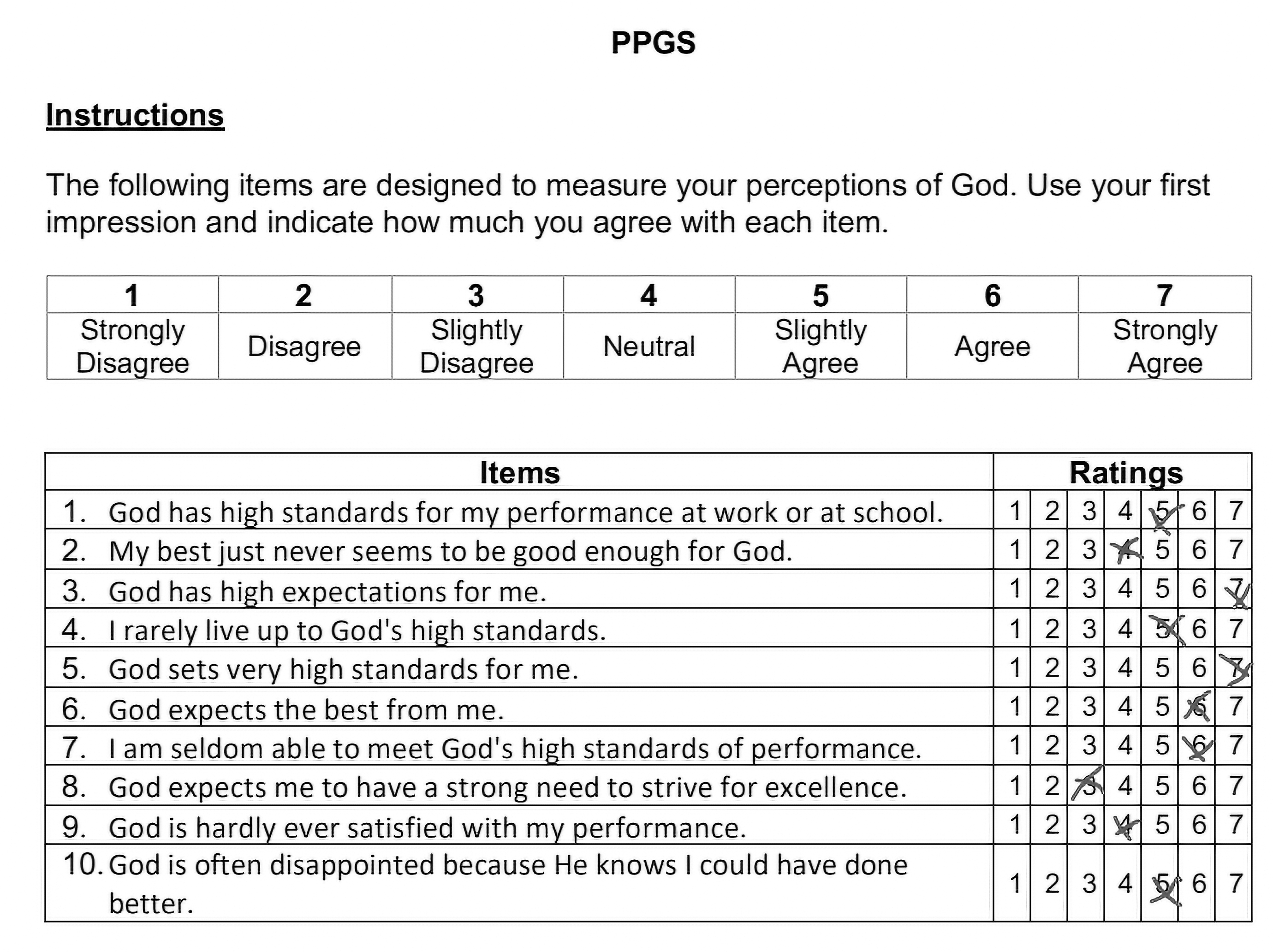
To assess the extremity of his religious perfectionism we used the Perceived Perfectionism from God Scale.64 Figures 4 through 6 show three administrations of this measure over the course of his treatment process, which focused almost entirely on the types of cognitive interventions outlined in this article. Just a visual scan of the images shows how this client shifted from an extreme all-or-nothing mentality about God (all of his answers hugging the right side of the scale) to a more flexible approach (his answers varying across the measure).
Figure 4. Perceived Perfectionism from God Scale, first client administration: January 30, 2020. Score = 67.
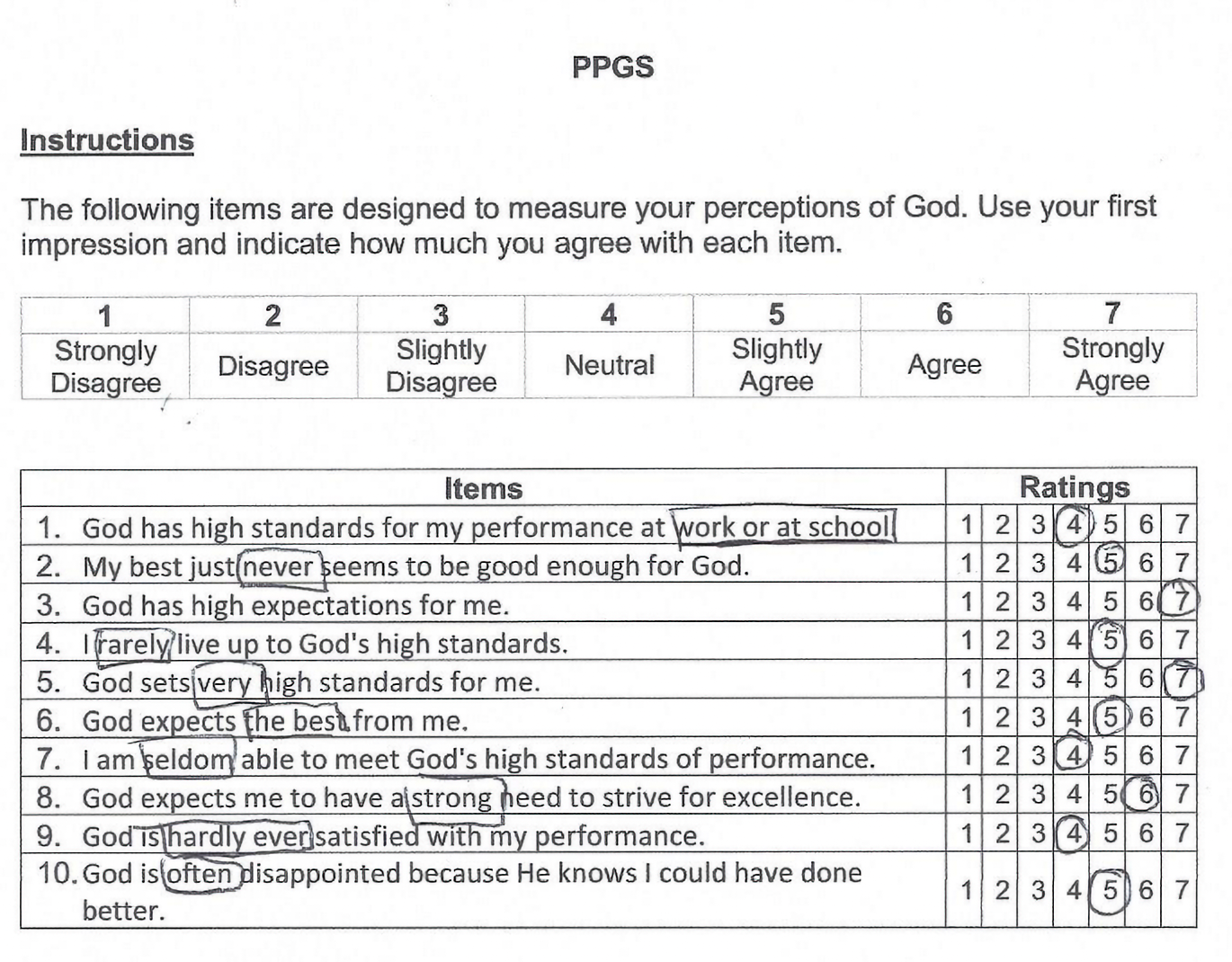
Figure 5. Perceived Perfectionism from God Scale, second client administration: October 15, 2020. Score = 52.
Figure 6. Perceived Perfectionism from God Scale, third client administration: April 29, 2021. Score = 52.
Even though his total scores on the measure were identical for administrations two and three, the range of answers varied more in the third administration, even hitting a three on the scale, which is a “slightly disagree” endorsement, representing a significant—even miraculous—milestone for him in his therapeutic journey. These images show the power of the cognitive work he did in treatment—over time, the rigidity of his unhealthy perfectionism broke down and became more flexible.
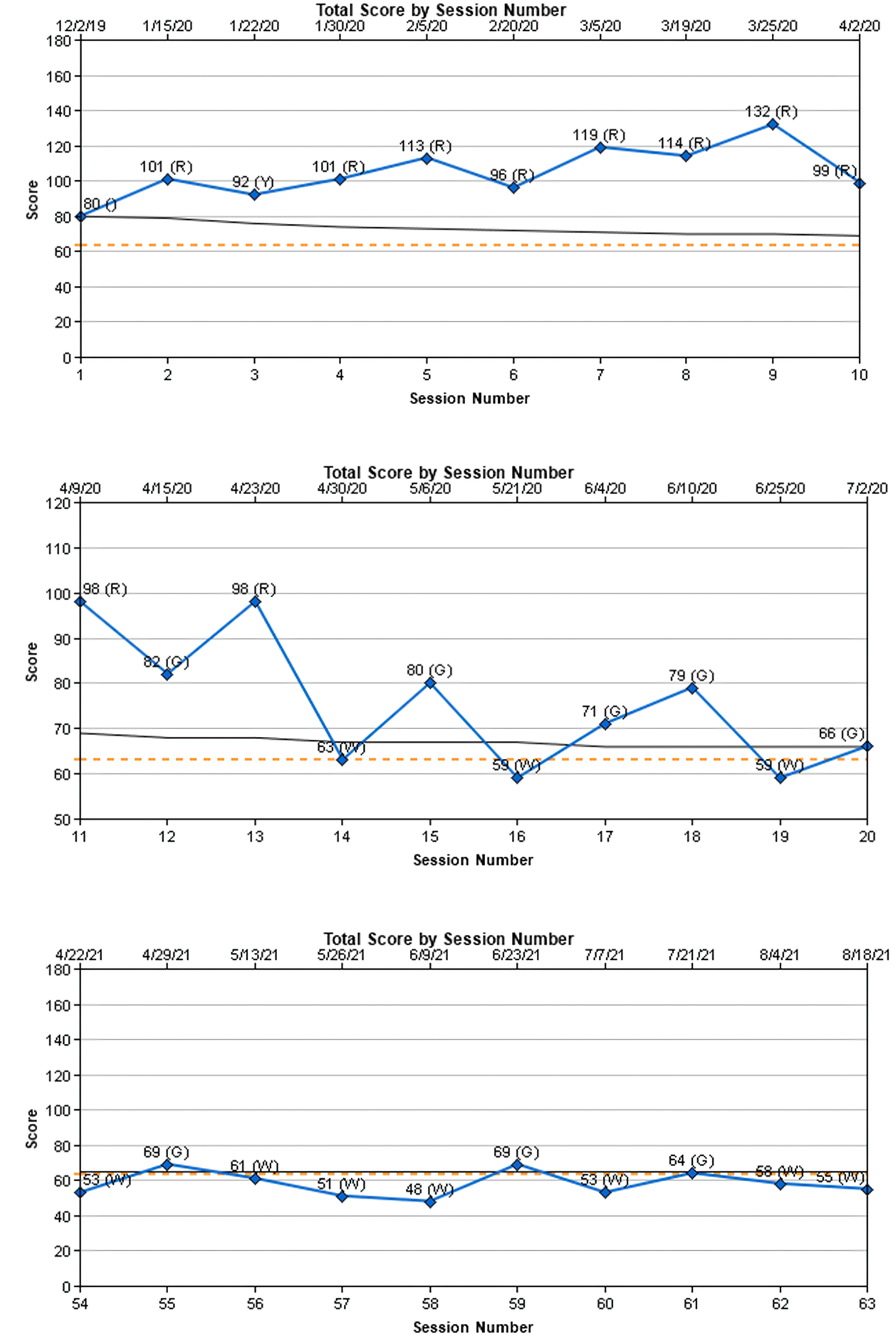
As his thinking became more flexible over the year and a half he spent in therapy, the intensity of his overall distress came down significantly. We used the Outcome Questionnaire 45.265 (OQ–45) to track his distress levels at each therapy session. The clinical cutoff score is 63, indicating that scores of 63 and above represent distress that is high enough to warrant targeted treatment. The average score for a nonclinical community population is 45, with scores below 62 falling in the average range. In figure 7, you can see several charts that show some of his OQ–45 scores. The first two charts show his first twenty data points from an assessment and then nineteen therapy sessions. His increasingly high distress scores over the first nine sessions illustrate how his distress increased as he got closer to a major deadline at work but did not yet have adequate therapeutic tools to deal with the stress in a healthy manner. You can see the sporadic nature of his distress during the next ten therapy sessions in the second chart as he began to gain some therapeutic skills and practice them. The third chart jumps ahead to show his functioning from sessions 54 to 63. At this time, he settled into a stable pattern of functioning, hovering around the clinical cutoff score, with most scores below the cutoff score in the normal range. From there, we continued to meet every three months (beyond what is shown in these charts) to allow him time to practice emotional self-reliance and maintain gains while still having some therapeutic accountability; his distress scores continued to remain low. After stabilizing for some time, he was emotionally self-reliant and resilient, and he was able to successfully discontinue treatment.
Figure 7. Outcome Questionnaire–45.2 charts for client.
At the end of his treatment process, this client reflected:
While there are therapeutic measures that show my progress, maybe my favorite measure is how my family sees me and responds to me. Just last week I reminded my seven-year-old how important it is to be flexible in her thinking, and she said, “That’s my dad!” I love that she sees me as a person who promotes flexible thinking in how we respond to life’s situations. After more than four years of avoiding temple worship (including while closed during the pandemic), I’ve recently returned, and I felt at peace. I’m able to think my way through most of my panic-inducing situations. I’ve even taken up some hobbies that include public performance, something inconceivable just a few years ago.
It’s been quite a journey. As I look back with compassion at my younger self, I wish I could let him know that help was on its way and that things would improve. I now understand that he was doing the best he could in the circumstances he was in. I did the best I could. I wasn’t perfect. But there is something beautiful to me in the dialectal beliefs that I wasn’t perfect, but I was doing the best I could, and it’s okay, and I was and am worthy of God’s love, and I can still grow and become better.
There is great power in trusting in the process. I’m so glad that I did. Two years ago, I was hiding in my bed, so depressed I couldn’t function. Today I’m happy, engaged in my life, and continuing to improve.66
The Commonality Between Gospel and Clinical Perspectives
Gospel teaching that can heal unhealthy perfectionism emphasizes setting aside self-defeating beliefs and distorted thinking, such as striving to earn worth and love from God or others with perfect behavior. Rather than a focus on negatively biased perfectionistic beliefs, the gospel focus remains on the Atonement of Jesus Christ. The gospel of Jesus Christ offers perfection in him and through him, even while we are imperfect or incomplete. We have faith in our Savior and accept that it is his perfection and healing that will ultimately perfect us in the eternities.
Clinical perspectives on healing from unhealthy perfectionism also emphasize becoming aware of and modifying negatively biased self-defeating beliefs and cognitive distortions. Clients shift distorted beliefs by identifying reality-based evidence they had previously ignored.
These two perspectives are not entirely distinct. It is not simply a choice between a gospel-centered approach or a clinical approach for treating unhealthy perfectionism. Do not both approaches expand a person’s perspective beyond their present interpretations and require cognitive flexibility to resist applying unhealthy perfectionistic assumptions? The approaches, when used together, can inform each other. For example, careful gospel study can provide data that helps promote cognitive restructuring. Clinical cognitive restructuring techniques also provide flexibility training to fully embrace and accept Christ’s teachings as he taught them—not as unhealthy perfectionism claims them to be. Enhancing cognitive flexibility allows those struggling to break perfectionistic perspectives and accept the errors and “grace” associated with mortal imperfection. This is illustrated by the following example.
One client struggled to listen to general conference talks by President Dallin H. Oaks. President Oaks’s professional history as a lawyer, a professor of law, and a justice of the Utah Supreme Court contributes to a professional delivery style that, coupled with her insecurities caused by unhealthy perfectionism, led her to believe that he was often condemning in his talks—because she felt condemned. I asked her to read a BYU devotional he gave in 1982 entitled “Our Strengths Can Become Our Downfall.”67 In this talk, President Oaks highlighted twenty strengths that, if not considered and navigated carefully, could be exploited by Satan and end up causing difficulty. As she talked about reading this discourse, she repeatedly used the phrase “President Oaks condemned . . .” I was struck by the strong negativity of the word she was using over and over again: “condemned.” I questioned her and even gently challenged her that I didn’t see anywhere in the discourse where President Oaks was condemning anybody. Instead, I saw that he was offering cautionary guidance to hopefully help prevent people from causing themselves serious problems. I sought to help her more accurately hear the message as it was being taught rather than hearing through the lens of her negative bias. She was genuinely surprised by my perspective and was struck by how negatively she interpreted something that didn’t come across negatively to me at all.
Then, to strengthen this more realistically based perspective that I presented, I introduced the cognitive technique of examining definitions. We talked about the difference between condemning someone and offering cautionary guidance to someone. We then went a step further with the cognitive emphasis. President Oaks has shared previously that his talks go through ten to fifteen drafts in the development phase,68 so the client and I discussed the idea that every word in his talks is there specifically for a chosen purpose. We examined the specific BYU devotional that had initially felt so condemning to her and his most recent general conference address. Words that would have made his messages demanding, harsh, or condemning were noticeably absent. He was not trying to scare anybody into behaving well. Instead, we found words that showed a purposeful softening of his message. Clearly, President Oaks wanted to make sure those listening felt encouraged and supported.
This cognitive intervention was eye-opening for her. She grew to see for herself how the meaning of President Oaks’s messages had become distorted by her unhealthy perfectionism. She continued to focus on the softening of his message for several weeks as she listened to more of his general conference talks and noticed the specific words he chose to use. As distortion in her thinking decreased, she began to feel the Spirit confirm the truthfulness of his words. The Spirit also helped her feel the love with which President Oaks gave his talks. This changed how she saw him. In a tremendous therapeutic reversal, this client no longer felt condemned by President Oaks’s talks and even grew to love listening to his talks in a very short amount of time. The loving feelings continued to expand as she kept listening to his talks with this new awareness, and in a few more weeks, she reported that she grew to “loving him so much.”69 The key was to engage more with the talks, not less, and strive to see things as they really were (Jacob 4:13).
Conclusion
Simply put, living the gospel of Jesus Christ in this mortal, fallen world as an imperfect human being requires us to rely on the atoning grace and mercy of our Lord and Savior Jesus Christ. While we strive to follow the gospel with good and honest hearts, perfect behavior is not possible and is not required for his atonement to have power in our lives. Our ability to accept this gift from him requires an intentional, flexible cognitive approach to daily living. By embracing flexibility through both gospel and clinical means, those struggling with unhealthy perfectionism can find emotional peace and freedom from the rigidity and condemnation of unhealthy perfectionistic beliefs and distortions.
Debra Theobald McClendon, PhD, is a licensed psychologist in the state of Utah and has interjurisdictional authorization to work with clients in most U.S. states. She specializes in treating those with scrupulosity, a religious and moral subtype of OCD. She is the owner of The OCD & Scrupulosity Clinic (ocdscrupulosityclinic.com) and is a member of the International OCD Foundation. She has been interviewed on podcasts, published articles, and published the book Freedom from Scrupulosity: Reclaiming Your Religious Experience from Anxiety and OCD (Religious Studies Center; Deseret Book, 2023).
2. Debra Theobald McClendon, “A Church Educator’s Guide to Identifying and Helping the Scrupulous Student,” Religious Educator 22, no. 2 (2021): 138–40. This section is reprinted with permission from the BYU Religious Studies Center. Minor revisions have been made.
3. Joachim Stoeber and Kathleen Otto, “Positive Conceptions of Perfectionism: Approaches, Evidence, Challenges,” Personality and Social Psychology Review 10, no. 4 (2006): 295–319.
4. Neal A. Maxwell, “Notwithstanding My Weakness,” Ensign 6, no. 11 (November 1976): 12–13.
5. Brandy A. Fedewa, Lawrence R. Burns, and Alex A. Gomez, “Positive and Negative Perfectionism and the Shame/Guilt Distinction: Adaptive and Maladaptive Characteristics,” Personality and Individual Differences 38, no. 7 (2005): 1609–19.
6. Fedewa, Burns, and Gomez, “Positive and Negative Perfectionism,” 1611.
8. G. E. Kawika Allen and Kenneth T. Wang, “Examining Religious Commitment, Perfectionism, Scrupulosity, and Well-Being Among LDS Individuals,” Psychology of Religion and Spirituality 6, no. 3 (2014): 262.
9. David Greenberg and Jonathan D. Huppert, “Scrupulosity: A Unique Subtype of Obsessive-Compulsive Disorder,” Current Psychiatry Reports 12 (2010): 286.
10. Jonathan S. Abramowitz and Ryan J. Jacoby, “Scrupulosity: A Cognitive-Behavioral Analysis and Implications for Treatment,” Journal of Obsessive-Compulsive and Related Disorders 3 (2014): 141.
11. Obsessive Compulsive Cognitions Working Group, “Cognitive Assessment of Obsessive-Compulsive Disorder,” Behaviour Research and Therapy 35, no. 7 (1997): 678.
12. Fedewa, Burns, and Gomez, “Positive and Negative Perfectionism,” 1611–12.
13. Fedewa, Burns, and Gomez, “Positive and Negative Perfectionism,” 1612.
14. Client story used with permission, also published in Debra Theobald McClendon, Freedom from Scrupulosity: Reclaiming Your Religious Experience from Anxiety and OCD (BYU Religious Studies Center; Deseret Book, 2023), 121.
15. Allan D. Rau, “‘Be Ye Therefore Perfect’: Beyond the Perfectionist Paradigm,” Religious Educator 12, no. 3 (2011): 38.
22. Ian Osborn, Can Christianity Cure Obsessive-Compulsive Disorder? A Psychiatrist Explores the Role of Faith in Treatment (Brazos Press, 2008), 160–61.
23. Osborn, Can Christianity Cure Obsessive-Compulsive Disorder?, 163.
24. See Russell N. Nelson, “Drawing the Power of Jesus Christ into Our Lives,” Ensign 47, no. 5 (May 2017): 39–42.
31. Russell M. Nelson, “Men’s Hearts Shall Fail Them,” The Church of Jesus Christ of Latter-day Saints, November 18, 2011, YouTube, 2:22–49, https://www.youtube.com/watch?v=EMwKxmTLaCs.
32. Handbook of Cognitive Behavioral Therapy: Overview and Approaches, ed. Amy Wenzel, vol. 1 (American Psychological Association, 2021), 207–34, https://doi.org/10.1037/0000218-008.
33. Martin M. Antony and Richard P. Swinson, When Perfect Isn’t Good Enough: Strategies for Coping with Perfectionism, 2nd ed. (New Harbinger Publications, 2009), 46.
34. David Burns, When Panic Attacks: The New, Drug-Free Anxiety Therapy That Can Change Your Life (Morgan Road Books, 2006), 99.
54. Justin D. Braun, Daniel R. Strunk, Katherine E. Sasso, and Andrew A. Cooper, “Therapist Use of Socratic Questioning Predicts Session-to-Session Symptom Change in Cognitive Therapy for Depression,” Behaviour Research and Therapy 70 (2015): 32–37, https://doi.org/10.1016/j.brat.2015.05.004; Egan and others, Cognitive-Behavioral Treatment, 113–15.
55. Egan and others, Cognitive-Behavioral Treatment, 163.
56. Egan and others, Cognitive-Behavioral Treatment, 164.
57. Egan and others, Cognitive-Behavioral Treatment, 166.
64. Kenneth T. Wang, G. E. Kawika Allen, Hannah I. Stokes, Han Na Suh, “Perceived Perfectionism from God Scale: Development and Initial Evidence,” Journal of Religion and Health 57 (2018): 2207–23, https://doi.org/10.1007/s10943-017-0405-1.
65. Michael J. Lambert, Ann T. Gregersen, and Gary M. Burlingame, “The Outcome Questionnaire–45,” in The Use of Psychological Testing for Treatment Planning and Outcomes Assessment, vol. 3, Instruments for Adults, ed. Mark E. Maruish, 3rd ed. (Lawrence Erlbaum Associates, 2004), 191–234.
66. Client story shared with permission. Also quoted in McClendon, Freedom from Scrupulosity, 212.